By Dr. Matthias Wiederholz with Performance Pain and Sports Medicine
Quadruple Board-Certified in Physical Medicine & Rehabilitation, Sports Medicine, Pain Medicine, and Regenerative Medicine
Updated February 12, 2026
Medically reviewed and updated for accuracy
Quick Insights
S2 nerve root compression symptoms typically include pain along the back of the thigh, numbness in the buttock or genital region, and in more severe cases, changes in bladder or bowel function. The S1 and S2 segments sit at the base of the spine within the sacrum, and disc pathology at this level is far less common than at L5-S1. However, when it does occur, identifying the exact nerve root involved is essential for guiding treatment. Many patients who search for S1-S2 disc problems are actually experiencing lumbosacral junction issues that affect the S1 or S2 nerve roots. Accurate diagnosis helps determine whether conservative care, interventional procedures, or regenerative approaches like the Discseel® Procedure offer the best path to relief.
Key Takeaways
- True disc herniation between S1 and S2 is anatomically rare because the sacral vertebrae are typically fused in adults. Most “S1-S2” symptoms originate from the lumbosacral junction (L5-S1) affecting sacral nerve roots.
- S2 nerve root compression produces a distinct symptom pattern, including posterior thigh numbness, perianal sensory changes, and potential bladder dysfunction, that differs from S1 compression.
- Bladder or bowel changes combined with saddle-area numbness may indicate cauda equina syndrome, which requires emergency medical evaluation.
- Non-surgical and minimally invasive interventional approaches can effectively manage most sacral nerve compression without the risks of lumbosacral fusion surgery.
Why It Matters
Pain radiating from the S1-S2 region can interfere with sitting, walking, sleeping, and daily activities that most people take for granted. Understanding whether your symptoms point to sacral nerve compression, disc pathology at the lumbosacral junction, or another cause helps you seek the right care sooner. Delayed diagnosis of sacral nerve involvement can lead to prolonged suffering or, in rare cases, permanent neurological changes. When you know what to look for and what questions to ask your physician, you take an active role in your recovery.
Introduction
As an interventional spine specialist, I evaluate patients every week who describe pain, numbness, or weakness that radiates from the low back into the buttock, thigh, or foot. Many arrive with imaging reports that reference the S1 or S2 nerve roots, and they understandably want to know what that means for their condition and their treatment options.
S2 nerve root compression symptoms can present differently from the more commonly discussed L5 or S1 radiculopathy patterns, and recognizing those differences matters for accurate diagnosis. This article is written for patients experiencing low back pain with sacral nerve involvement, whether the underlying cause is a disc herniation at the lumbosacral junction, degenerative changes, or less common sacral pathology. You can explore a full overview of advanced disc treatment options available at our practice, including regenerative procedures designed to repair disc damage at its source.
I invite you to review my professional background to understand the comprehensive, evidence-based approach I take to diagnosing and treating complex spine conditions at Performance Pain and Sports Medicine.

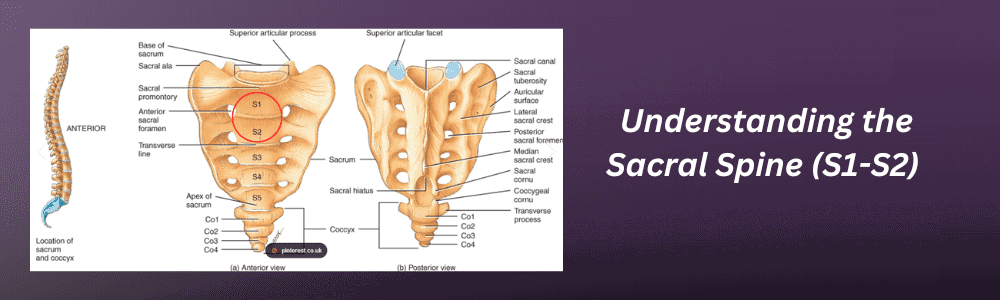
Where Are S1 and S2 on the Spine?
The sacrum sits at the very base of the spinal column, just below the five lumbar vertebrae and above the coccyx (tailbone). It is a triangular bone formed by five vertebral segments, labeled S1 through S5, that gradually fuse together during adolescence and early adulthood. By the time most people reach their mid-twenties, these segments have fused into a single solid structure.
The S1 vertebra is the largest and most superior segment of the sacrum. It articulates directly with the fifth lumbar vertebra (L5) at the lumbosacral junction, forming one of the most biomechanically stressed transitions in the entire spine. This junction bears the full weight of the upper body and absorbs significant forces during bending, lifting, and twisting. The S2 vertebra sits just below S1 and is slightly smaller, contributing to the sacrum’s overall wedge shape that locks into the pelvis at the sacroiliac joints.
Both S1 and S2 have openings called sacral foramina through which nerve roots exit the spinal canal. These nerve roots contribute to the sacral plexus, which provides motor and sensory function to the lower limbs, pelvic floor, bladder, and bowel. The sacrum also connects to the pelvis through the sacroiliac joints, and a network of ligaments, including the sacrospinous and sacrotuberous ligaments, provides structural stability for weight transfer from the spine to the legs. Research into sacral causes of radiculopathy confirms that understanding this anatomy is essential for differentiating disc-related nerve compression from other sources of sacral pain.
S1-S2 Herniated Disc Symptoms: What Patients Actually Experience
One of the most important clinical points about this topic is that true disc herniation between the S1 and S2 vertebrae is extremely rare in adults. Because the sacral segments fuse during development, there is typically no functional intervertebral disc between S1 and S2 by adulthood. When patients or imaging reports reference “S1-S2 symptoms,” they are most often describing pathology at the L5-S1 disc level that compresses the S1 or S2 nerve roots as they travel through the spinal canal and exit through the sacral foramina.
This distinction matters because the treatment approach depends on identifying the true source of nerve irritation. Disc herniations at L5-S1 are among the most common in the lumbar spine, and they can produce symptoms that patients associate with the sacral region. Those symptoms typically include localized low back pain that may radiate into the buttock, posterior thigh, and calf. Many patients also experience numbness or tingling along the outer foot and sole, reduced ankle reflex, and difficulty with toe-off strength during walking.
In less common cases where sacral pathology does exist, such as a sacral Tarlov cyst or a transitional vertebra with a residual disc element, the symptom pattern may overlap with what is described above but can also include deeper pelvic pain, perineal discomfort, and more diffuse sensory changes. S1 nerve root compression specifically tends to affect the calf, heel, and lateral foot, while S2 involvement more often affects the posterior thigh, buttock, and saddle area.
S2 Nerve Root Compression Symptoms: How This Nerve Root Differs
The S2 nerve root has specific responsibilities that produce a recognizable pattern when it becomes compressed or irritated. According to established dermatomal mapping references, the S2 dermatome covers the posterior thigh, the back of the calf, and portions of the perineum and genital area. This means S2 nerve root compression symptoms can look quite different from the more familiar L5 or S1 patterns that many patients and even some clinicians initially consider.
Patients with S2 involvement commonly report numbness or a burning sensation along the back of the upper leg and into the buttock crease. Some experience altered sensation in the perineal or genital region, which can be distressing and is often underreported. The S2 nerve root also contributes to bladder and bowel control through the sacral parasympathetic outflow. When compression is significant, patients may notice urinary urgency, difficulty initiating urination, or a sensation of incomplete bladder emptying.
Motor involvement from S2 compression is often subtle. Patients may notice some weakness in the hamstring muscles or difficulty with certain movements of the foot, though these deficits are typically less pronounced than the calf weakness seen with S1 compression. Reflex changes can include diminished ankle jerk, though this finding overlaps with S1 pathology and requires careful clinical correlation.
It is worth noting that the sacral nerve roots travel together as part of the cauda equina within the spinal canal before exiting through the sacral foramina. This means that pathology at the lumbosacral junction can affect multiple sacral nerve roots simultaneously, producing a broader symptom pattern than a single isolated root compression would suggest.
S2 Nerve Damage vs. Nerve Compression: Knowing the Difference
Patients often use the terms “nerve damage” and “nerve compression” interchangeably, but these represent different stages of nerve involvement with different implications for recovery. Compression refers to mechanical pressure on the nerve root, typically from a herniated disc, bone spur, or narrowed foramen. When the compression is relieved, either through natural resorption of disc material or through intervention, the nerve can often recover its normal function.
Nerve damage, by contrast, implies that the nerve fibers themselves have sustained structural injury. This can occur when compression is severe and prolonged, when inflammatory chemicals from a leaking disc cause chemical radiculitis, or when blood supply to the nerve root is compromised. A systematic review of diagnostic accuracy for lumbosacral radiculopathy highlights the importance of distinguishing these presentations through careful clinical examination and electrodiagnostic testing.
Warning signs that S2 nerve compression may be progressing toward more significant nerve injury include progressive numbness that does not fluctuate, persistent weakness that worsens over days or weeks, and new onset of bladder or bowel dysfunction. These findings warrant prompt medical evaluation because early intervention can prevent permanent neurological deficits.

When S1-S2 Symptoms Require Emergency Attention
While most sacral nerve compression follows a gradual course and responds to conservative or interventional treatment, certain symptom combinations indicate a potential emergency. Cauda equina syndrome occurs when multiple nerve roots at the base of the spinal canal become severely compressed, and it can result in permanent bladder, bowel, and sexual dysfunction if not treated within hours.
A guideline-oriented review of cauda equina red flags and triage protocols emphasizes that the following symptoms should prompt immediate emergency evaluation: new onset of urinary retention or inability to sense when the bladder is full, loss of sensation in the “saddle” area (inner thighs, perineum, and buttocks), bilateral leg weakness or numbness, and progressive loss of bowel control. These symptoms can develop suddenly after an acute disc herniation or gradually from a slowly expanding mass.
If you experience any combination of these symptoms, go to the nearest emergency department immediately. Cauda equina syndrome is rare, but recognizing it early makes a significant difference in outcomes. Your emergency physician will typically order an urgent MRI to evaluate the degree of nerve compression and determine whether surgical decompression is necessary.
How S1-S2 Disc Problems Are Diagnosed
Accurate diagnosis of sacral nerve compression begins with a thorough clinical history and physical examination. Your physician will ask about the specific location of your pain, numbness, and weakness. Certain tests performed during the physical examination, such as the straight leg raise, ankle reflex testing, and sensory testing along specific dermatomes, help identify which nerve root is involved.
Magnetic resonance imaging (MRI) is the primary imaging tool for evaluating disc pathology and nerve compression at the lumbosacral junction. MRI can visualize disc herniations, foraminal narrowing, and other structural changes that compress the sacral nerve roots. In some cases, a CT scan may provide additional detail about bony anatomy, particularly if spinal stenosis or sacral fracture is suspected.
Electrodiagnostic studies, including nerve conduction studies and electromyography (EMG), can confirm which nerve root is affected and help distinguish active nerve compression from resolved or chronic changes. These tests measure the electrical activity of muscles supplied by specific nerve roots and can detect subtle denervation patterns that clinical examination alone may miss.
Diagnostic injections also play an important role in confirming pain generators. Selective nerve root blocks, epidural injections, or sacroiliac joint injections can help your physician determine whether the sacral nerve roots, the facet joints, or the sacroiliac joints are the primary source of symptoms. This targeted approach guides treatment decisions and avoids unnecessary procedures directed at the wrong structure.
Treatment Options for S1-S2 Nerve Compression
For most patients with sacral nerve compression, treatment begins with conservative measures and progresses to interventional options when needed. The goal at every stage is to reduce nerve irritation, restore function, and address the underlying cause of compression. A comprehensive review of lumbar radiculopathy diagnosis and treatment confirms that the majority of patients with radiculopathy improve with non-surgical management, though the timeline varies depending on the severity of compression.
Conservative Care
Physical therapy focused on core stabilization and lumbar mobility can reduce mechanical stress on the lumbosacral junction. Anti-inflammatory medications, neuropathic pain medications, and short courses of oral corticosteroids may help manage acute flare-ups. Activity modification, including avoiding prolonged sitting and heavy lifting during the acute phase, allows inflamed tissues to begin healing while maintaining gentle movement to prevent deconditioning.
Interventional Pain Management
When conservative measures provide incomplete relief, targeted interventional procedures can deliver more focused treatment. Research on peripheral nerve blocks for lumbosacral radiculopathy demonstrates the value of outpatient interventional approaches in managing chronic sacral nerve pain. Epidural steroid injections deliver anti-inflammatory medication directly to the compressed nerve root. Selective nerve root blocks can provide both diagnostic information and therapeutic benefit. Radiofrequency ablation may be considered for facet-mediated pain contributing to the overall symptom pattern.
The Discseel® Procedure for S1-S2 Disc Damage
For patients whose symptoms stem from structural disc damage, specifically annular tears that allow inflammatory material to leak and irritate nearby nerve roots, the Discseel® Procedure offers a fundamentally different approach. Rather than removing disc material or fusing vertebrae, this minimally invasive treatment uses a biologic fibrin sealant to seal annular tears and stimulate natural collagen regeneration within the damaged disc.
The procedure begins with a diagnostic annulogram that identifies actively leaking discs under fluoroscopic guidance. The fibrin sealant is then injected into the affected discs, where it mechanically seals tears and creates a scaffold for new tissue growth. Over time, the fibrin is absorbed and replaced with regenerated collagen, restoring structural integrity to the disc. This approach preserves spinal mobility and addresses the root cause of discogenic pain rather than just managing symptoms.
Dr. Matthias Wiederholz was the first physician in Houston to perform the Discseel® Procedure and was personally trained by Dr. Kevin Pauza, the procedure’s inventor. As one of only three certified master instructors worldwide, Dr. Wiederholz brings unmatched expertise to evaluating whether patients with lumbosacral disc pathology are candidates for this regenerative approach.
Wondering if the Discseel® Procedure might be right for your S1-S2 disc pain?
Complete our brief intake form to find out if you may be a candidate. Dr. Wiederholz personally reviews each submission to determine whether your condition may respond to biologic disc repair.
Recovery and Rehabilitation After S1-S2 Treatment
Recovery from sacral nerve compression depends on the treatment approach used and the duration and severity of the original compression. Patients who respond to conservative care or interventional injections often notice improvement within weeks, though complete resolution may take several months as the nerve heals and inflammation subsides.
Following any interventional procedure, structured rehabilitation helps optimize outcomes. Core strengthening exercises that target the deep stabilizers of the lumbar spine and pelvis can reduce ongoing mechanical stress on the lumbosacral junction. Gentle flexibility work, including hip stretches and sciatic nerve glides, can improve mobility without aggravating the healing nerve root. Low-impact aerobic activities like walking, swimming, or stationary cycling support cardiovascular health while minimizing spinal loading.
Proper body mechanics during daily activities play an important role in preventing recurrence. Learning to lift with the legs rather than the back, avoiding prolonged static postures, and maintaining a healthy body weight all reduce the cumulative stress on lumbosacral discs and nerve roots. Your physical therapist can guide you through a graduated return to full activity, adjusting the program based on your symptom response at each stage.
For patients who undergo the Discseel® Procedure, the recovery timeline follows a specific protocol. Most patients begin walking the day after treatment. Activity restrictions are gradually lifted over several weeks as the fibrin sealant integrates and collagen regeneration progresses. Full recovery typically takes several months, during which time patients work closely with our team to monitor progress and optimize rehabilitation.
Conclusion
S1-S2 spine symptoms, whether from disc pathology at the lumbosacral junction or from sacral nerve root compression, deserve accurate diagnosis and targeted treatment. The S2 nerve root serves specific functions related to sensation in the posterior thigh, pelvic floor control, and bladder function, and identifying its involvement shapes the entire treatment plan. While true disc herniation between the fused sacral vertebrae is rare, the nerve roots that exit through this region are frequently affected by conditions originating at the L5-S1 level.
Conservative care, interventional pain management, and regenerative procedures like the Discseel® Procedure each play a role depending on the severity and source of nerve compression. The key is working with a physician who can accurately identify the pain generator, differentiate between compression and nerve damage, and create a treatment plan tailored to your specific anatomy and goals.
If you are experiencing persistent low back pain with radiating leg symptoms, numbness, or any changes in bladder or bowel function, I encourage you to seek evaluation sooner rather than later. At our Houston location, we use advanced diagnostic tools to identify the exact source of your symptoms and develop a personalized plan that prioritizes your long-term function and quality of life. Contact our team to schedule your consultation.
Ready to find answers for your sacral spine pain?
Submit our Discseel® intake form or call our Houston office at 346-217-1111 to start your evaluation today.
This article is for educational purposes only and should not be used as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition or treatment options. Never disregard professional medical advice or delay in seeking it because of something you have read in this article.
Frequently Asked Questions
What does S2 nerve pain feel like?
S2 nerve pain typically presents as a burning, aching, or shooting sensation along the back of the thigh and into the buttock. Some patients also report numbness or tingling in the perineal region. Unlike the classic sciatica pattern that radiates down the back of the calf and into the foot (more typical of S1 compression), S2 pain tends to remain more proximal and may involve deeper pelvic discomfort. Each patient’s experience varies depending on the degree of nerve irritation and whether compression is partial or complete.
Can you actually herniate a disc between S1 and S2?
True disc herniation between S1 and S2 is extremely uncommon in adults because the sacral vertebrae fuse into a single bone during development. By the mid-twenties, there is typically no functional disc remaining between these segments. Most patients diagnosed with “S1-S2 symptoms” actually have disc pathology at the L5-S1 level that compresses the S1 or S2 nerve roots as they travel through the spinal canal. Rare exceptions include transitional vertebrae, where an extra lumbar segment creates a disc space at the lumbosacral junction, or sacral Tarlov cysts that affect the sacral nerve roots.
How long does S2 nerve root compression take to heal?
Recovery timelines vary significantly depending on the cause and severity of compression. Mild compression from a small disc protrusion may improve within six to twelve weeks with conservative care. More significant herniations can take several months to resolve, particularly if the nerve root was compressed for an extended period before treatment began. Patients with documented nerve damage on electrodiagnostic testing may require longer recovery periods. Working with a spine specialist to monitor progress ensures that treatment can be adjusted if recovery stalls.
When should I go to the ER for sacral spine symptoms?
Seek emergency medical attention if you develop sudden loss of bladder or bowel control, inability to sense when your bladder is full, numbness in the “saddle” area between your thighs, or rapidly progressive weakness in both legs. These symptoms may indicate cauda equina syndrome, which requires urgent imaging and potentially emergency surgery to prevent permanent nerve damage. While this condition is rare, timely intervention within hours of symptom onset significantly improves outcomes.
What is the difference between S1 and S2 nerve compression symptoms?
S1 nerve root compression typically causes pain radiating down the back of the calf, numbness along the outer foot and sole, weakness in calf muscles (difficulty with toe raises), and a diminished ankle reflex. S2 nerve root compression more often produces posterior thigh and buttock pain, numbness in the perineal area, and potential bladder or bowel changes due to the S2 root’s contribution to pelvic organ function. In practice, these patterns often overlap because disc pathology at the lumbosacral junction can affect both nerve roots simultaneously.
Is the Discseel® Procedure an option for sacral disc problems?
The Discseel® Procedure may be an option for patients whose symptoms arise from annular tears and disc damage at the lumbosacral junction (L5-S1), which is the most common source of sacral nerve root compression. During the diagnostic annulogram, Dr. Wiederholz identifies which discs are actively leaking inflammatory material. If the L5-S1 disc is the confirmed pain generator, the biologic fibrin sealant can be applied to seal the tears and promote disc healing. Candidacy depends on your specific imaging findings, symptom pattern, and response to prior treatments.















