By Dr. Matthias Wiederholz with Performance Pain and Sports Medicine
Quadruple Board-Certified in Physical Medicine & Rehabilitation, Sports Medicine, Pain Medicine, and Regenerative Medicine
Updated January 29, 2026
Medically reviewed and updated for accuracy
Quick Insights
The S1 nerve originates from the first sacral vertebra and forms a major component of the sciatic nerve. It controls plantar flexion (pointing your foot downward), provides sensation to the lateral foot and heel, and generates the Achilles reflex. When compressed at the L5-S1 junction—often by disc herniation or stenosis—patients experience pain radiating down the back of the leg to the outer foot, along with weakness pushing off while walking. Understanding S1 nerve distribution helps identify the source of lower extremity symptoms and guides targeted interventional treatments.
Introduction
The S1 nerve plays a fundamental role in lower body function, yet many patients experiencing radiating leg pain don’t fully understand where this nerve originates or what it controls. In my interventional spine practice in Houston and Lawrenceville, I frequently evaluate patients with S1 nerve-related symptoms—typically pain that travels from the lower back down the posterior leg to the lateral aspect of the foot.
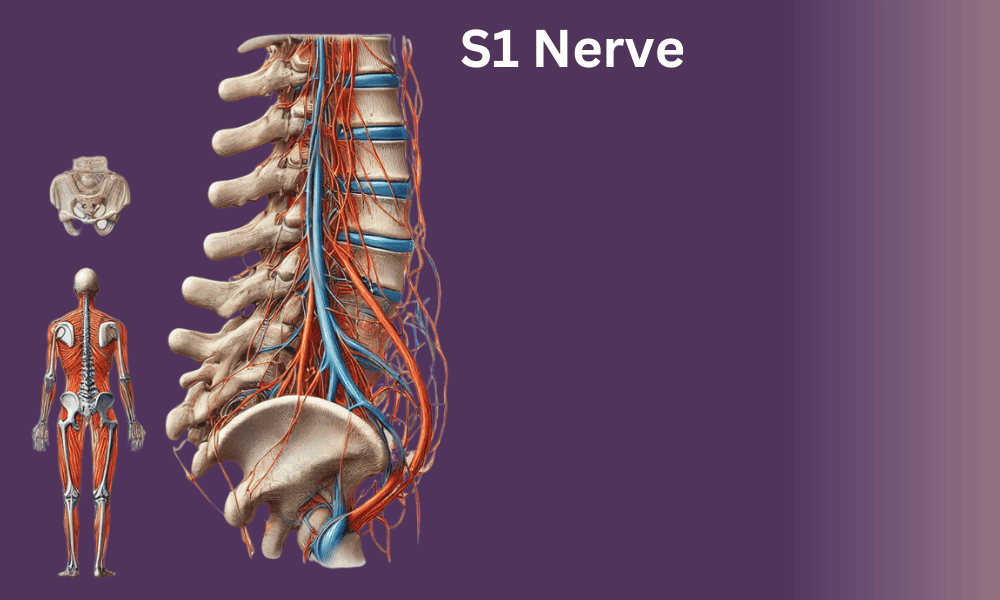
The S1 nerve emerges from the first sacral vertebra, located at the base of your spine where the lumbar vertebrae transition into the fused sacral bones. This nerve root exits the spinal canal and joins with other lumbosacral nerve roots to form the sciatic nerve, which is the largest nerve in your body. The lumbosacral plexus, including S1 contributions, supplies motor and sensory innervation to the entire lower extremity.
What makes S1 nerve compression clinically significant is its location at the L5-S1 disc level—the most common site of lumbar disc herniation and degenerative changes. When disc material or bone spurs compress the S1 nerve root, the resulting symptoms follow a predictable distribution pattern. However, clinical research shows that dermatomal pain patterns are not always reliable for diagnosis, with individual variation being more common than textbook presentations.
This article explains S1 nerve anatomy, its pathway through the lower body, the motor and sensory functions it controls, and how S1 nerve root compression manifests clinically. For patients with confirmed disc pathology at L5-S1 causing persistent S1 radiculopathy, we offer advanced interventional options including the Discseel® Procedure—a biologic approach to sealing annular tears and supporting natural disc healing.
You can learn more about my background as a Master Instructor in the Discseel® Procedure and how this training informs my approach to lumbosacral nerve pathology.

Where Is S1 on the Spine? Understanding Sacral Anatomy
The S1 vertebra is located at the top of your sacrum—the triangular bone at the base of your spine that forms the posterior wall of your pelvis. To understand where S1 sits, picture your spine divided into regions: seven cervical (neck) vertebrae, twelve thoracic (mid-back) vertebrae, five lumbar (lower back) vertebrae, and then the sacrum.
The sacrum itself consists of five vertebrae (S1 through S5) that fuse together during development into a single bone. S1 is the uppermost sacral segment and sits directly below the L5 vertebra. The junction between L5 and S1—referred to as the L5-S1 disc space—bears tremendous mechanical stress because it represents the transition point between the mobile lumbar spine and the fixed sacrum.
This L5-S1 junction is where the S1 nerve root exits the spinal canal. Specifically, the S1 nerve emerges through the first sacral foramen (a bony opening on each side of the sacrum). Anatomical studies of lumbosacral nerve roots show that the S1 root typically travels a short intrathecal course before exiting, and its size and trajectory can vary between individuals.
When patients ask “where is S1,” I often explain it this way: if you place your hand on your lower back and move down toward your tailbone, you’ll feel a bony prominence—that’s the top of your sacrum, where S1 is located. The L5-S1 disc sits just above this point. Because this area supports your entire upper body weight and experiences significant flexion-extension forces, it’s highly susceptible to disc degeneration and herniation that can compress the S1 nerve root.
S1 Nerve Pathway and Distribution: From Spine to Lower Limb
After the S1 nerve root exits through the sacral foramen, it joins with the L4, L5, and other sacral nerve roots to form the sacral plexus within the pelvis. The sacral plexus gives rise to several major nerves, most notably the sciatic nerve.
The S1 nerve root contributes significantly to the sciatic nerve, which is formed by nerve roots L4 through S3. This large nerve exits the pelvis through the greater sciatic foramen (below the piriformis muscle) and descends down the posterior thigh. As it travels, the sciatic nerve carries both motor signals (to activate muscles) and sensory signals (to transmit pain, temperature, and touch sensations back to the brain).
In the lower thigh, the sciatic nerve typically divides into two terminal branches: the tibial nerve and the common peroneal nerve. The S1 nerve root contributes primarily to the tibial nerve division, which continues down the back of the leg and into the foot. This is why S1 radiculopathy produces symptoms along the posterior and lateral leg rather than the anterior leg.
Understanding this pathway is crucial because symptom referral patterns during nerve root irritation often diverge from classic dermatomal maps. In clinical practice, S1 nerve compression at the spinal level can cause pain anywhere along this distribution—from the lower back and buttock, down the posterior thigh, into the calf, and radiating to the lateral foot and heel.
The S1 dermatomal distribution includes the lateral aspect of the foot (including the fourth and fifth toes), the heel, and the sole of the foot. However, studies examining L5 and S1 nerve compressions demonstrate that actual patient-reported pain patterns frequently extend beyond traditional dermatome boundaries, with considerable individual variation.
What Does the S1 Nerve Control? Motor and Sensory Functions
The S1 nerve root controls several critical motor and sensory functions in your lower body. Understanding these functions helps both patients and clinicians recognize S1 nerve involvement when symptoms appear.
Motor Functions (Muscle Control)
The S1 nerve primarily innervates muscles involved in plantar flexion—the movement of pointing your foot downward. The major muscles controlled by S1 include:
- Gastrocnemius and soleus muscles: These calf muscles are the primary plantar flexors. When you stand on your tiptoes or push off while walking, you’re using S1-innervated muscles. Weakness in these muscles makes it difficult to perform heel raises or walk with a normal gait.
- Gluteus maximus: The S1 nerve contributes to hip extension (moving your thigh backward). Weakness here can affect climbing stairs or rising from a seated position.
- Hamstring muscles: While primarily innervated by the sciatic nerve’s L5 and S1 components, hamstring function depends partly on S1 for knee flexion (bending your knee).
Clinically, when I evaluate patients for S1 nerve function, I ask them to perform a heel raise test—standing on one leg and lifting the heel off the ground. Inability to do this, or weakness compared to the opposite side, suggests S1 motor compromise.
Sensory Functions (Feeling and Sensation)
The S1 nerve provides sensation to specific areas of the lower limb:
- Lateral foot and fifth toe: The outer edge of your foot and your smallest toe receive sensory input from S1.
- Heel and sole: The bottom of your foot, particularly the heel region, is innervated by S1 nerve branches.
- Posterior calf: Sensation along the back of the lower leg is partially S1-mediated.
- Lateral ankle: The outer aspect of your ankle area receives S1 sensory innervation.
When S1 nerve compression occurs, patients often report numbness, tingling (paresthesias), or altered sensation in these regions. Some describe a “pins and needles” feeling or a sensation that their foot has “fallen asleep.” Dermatomal maps illustrate these distributions, though as noted, actual clinical presentations vary.
Reflex Testing: The Achilles Reflex
The S1 nerve root mediates the Achilles tendon reflex (also called the ankle jerk reflex). When a reflex hammer taps the Achilles tendon, the calf muscles should contract reflexively, causing plantar flexion of the foot. This reflex arc travels through the S1 nerve root—sensory signals go up to the spinal cord at the S1 level, and motor signals come back down through the same root.
A diminished or absent Achilles reflex is a classic sign of S1 nerve root pathology. During physical examination, I routinely test this reflex bilaterally. An asymmetric or absent reflex on one side strongly suggests S1 nerve compromise on that side, often due to disc herniation or foraminal stenosis at L5-S1.

S1 Nerve Root Anatomy: Exit Point and Foraminal Relationships
To fully understand S1 nerve pathology, it’s important to know the anatomy of where the nerve exits the spinal canal. The S1 nerve root exits through the S1 neural foramen—a bony opening formed by the pedicles of the L5 and S1 vertebrae, the L5-S1 disc anteriorly, and the facet joint posteriorly.
This foramen is where compression most commonly occurs. When the L5-S1 disc herniates posterolaterally, disc material can protrude into the neural foramen or lateral recess, directly compressing the exiting S1 nerve root. Similarly, as the L5-S1 facet joints degenerate and enlarge (facet hypertrophy), they can narrow the foramen and pinch the S1 nerve.
The intrathecal portion of the S1 nerve root—the segment inside the dural sac before it exits—typically travels along the posterior aspect of the vertebral body. Anatomical research has documented considerable variability in nerve root size, number of rootlets, and intradural course. This variability helps explain why some patients with similar-appearing disc herniations on MRI have vastly different symptom severity.
Understanding foraminal anatomy is critical when performing interventional procedures. For example, when I perform a transforaminal epidural steroid injection targeting the S1 nerve, I use fluoroscopic guidance to position the needle precisely at the S1 foramen opening. The goal is to deliver anti-inflammatory medication directly to the inflamed nerve root, reducing chemical irritation and mechanical compression effects.
Clinical Presentation of S1 Radiculopathy
S1 radiculopathy refers to symptoms caused by S1 nerve root irritation or compression. Patients typically present with a constellation of findings that align with the nerve’s distribution and function. However, it’s important to recognize that pain patterns in radiculopathy don’t always follow textbook dermatomal maps—S1 radicular pain is somewhat more consistent with its dermatome than other lumbar levels, but variability remains significant.
Common Symptoms of S1 Nerve Compression
Patients with S1 nerve root compression typically report:
- Radiating pain: Sharp, burning, or electric-like pain starting in the lower back or buttock and traveling down the posterior thigh, into the calf, and radiating to the lateral foot and heel. The pain often worsens with prolonged sitting, forward bending, or Valsalva maneuvers (coughing, sneezing, bearing down).
- Numbness and tingling: Patients describe altered sensation along the S1 distribution—particularly the lateral foot, fifth toe, heel, and sole. Some report a “dead” feeling in these areas or persistent tingling.
- Weakness: Difficulty standing on tiptoes, pushing off while walking, or performing heel raises. Patients may notice they can’t walk normally or that their affected leg feels heavy.
- Reduced or absent Achilles reflex: This finding on physical exam is nearly pathognomonic for S1 radiculopathy.
- Worsening with activity: Symptoms often intensify with walking, standing, or activities that load the lumbar spine, while lying flat may provide temporary relief.
Differentiating S1 from L5 Radiculopathy
Because L5 and S1 nerve issues can present similarly, distinguishing between them is important for diagnosis. Key differences include:
- Sensory distribution: L5 radiculopathy affects the top of the foot and the first web space (between big toe and second toe), while S1 radiculopathy affects the lateral foot and fifth toe.
- Motor findings: L5 weakness causes foot drop (difficulty lifting the foot upward), whereas S1 weakness causes difficulty with plantar flexion (pushing the foot downward).
- Reflex changes: L5 radiculopathy typically doesn’t affect reflexes, while S1 radiculopathy reduces or abolishes the Achilles reflex.
In practice, some patients have multilevel disc disease affecting both L5 and S1 roots, producing overlapping symptoms that require careful neurological examination and imaging correlation to sort out.

Diagnostic Evaluation for S1 Nerve Pathology
Accurate diagnosis of S1 nerve compression requires integration of clinical findings, physical examination, and advanced imaging. In my practice, I use a systematic approach to confirm the diagnosis before recommending treatment.
Physical Examination
During the physical exam, I assess:
- Motor strength testing: Heel raises (single-leg and bilateral), hip extension, and knee flexion strength.
- Sensory examination: Light touch and pinprick testing along the S1 dermatome, comparing both sides.
- Reflex testing: Achilles tendon reflex bilaterally. An absent or diminished reflex on one side is significant.
- Provocative maneuvers: Straight leg raise test (reproducing radiating leg pain by lifting the extended leg) and slump test to assess nerve root tension.
These examination findings, when consistent with S1 nerve distribution, help localize the pathology and guide imaging.
MRI of the Lumbar Spine
Magnetic resonance imaging (MRI) is the gold standard for visualizing soft tissue structures affecting the S1 nerve root. MRI can identify:
- Disc herniation at L5-S1: Posterior or posterolateral disc protrusion compressing the S1 nerve root in the lateral recess or neural foramen.
- Foraminal stenosis: Narrowing of the S1 neural foramen due to disc space collapse, facet hypertrophy, or ligamentum flavum thickening.
- Annular tears: High-intensity zones on T2-weighted images indicating fissures in the disc’s outer layer, which can be a source of discogenic pain and inflammatory nerve irritation.
- Nerve root enhancement: On contrast-enhanced MRI, an inflamed S1 nerve root may show abnormal enhancement, indicating active inflammation.
It’s important to correlate imaging findings with clinical symptoms. Not all disc herniations visible on MRI cause symptoms—some are incidental findings in asymptomatic individuals.
CT Myelography
When MRI is contraindicated (e.g., patients with pacemakers or severe claustrophobia), CT myelography provides an alternative. This involves injecting contrast dye into the spinal canal and then obtaining CT images. It effectively shows nerve root compression, though it’s more invasive than MRI.
Electrodiagnostic Studies
Electromyography (EMG) and nerve conduction studies can confirm S1 nerve root dysfunction and differentiate it from peripheral nerve problems. These studies measure electrical activity in muscles and nerves, helping determine:
- Whether there is active denervation (muscle changes due to nerve injury)
- The severity and chronicity of nerve damage
- Whether multiple nerve roots are involved
While EMG isn’t always necessary for straightforward cases, it’s valuable when the clinical picture is unclear or when differentiating radiculopathy from peripheral neuropathy.

Treatment Approaches for S1 Nerve Compression
Treatment for S1 nerve compression depends on symptom severity, functional impairment, imaging findings, and patient goals. I typically follow a stepwise approach, starting with conservative measures and advancing to interventional or surgical options when indicated.
Conservative Management
Most patients with S1 radiculopathy improve with conservative care over 6-12 weeks. Initial management includes:
- Activity modification: Avoiding activities that exacerbate symptoms (prolonged sitting, heavy lifting, forward bending).
- Physical therapy: Focused on core strengthening, lumbar stabilization, and nerve gliding exercises to reduce tension on the S1 nerve root.
- Medications: Nonsteroidal anti-inflammatory drugs (NSAIDs) for inflammation, neuropathic pain medications (gabapentin, pregabalin) for nerve-related pain, and short-term muscle relaxants if muscle spasm is present.
- Heat and ice therapy: Alternating applications to reduce muscle spasm and inflammation.
Conservative treatment works well for many patients, particularly those with acute radiculopathy from disc herniation that hasn’t caused significant weakness.
Interventional Pain Management
When conservative treatment doesn’t provide adequate relief, or when symptoms significantly impair function, interventional procedures can target the inflamed nerve root directly:
Epidural Steroid Injections
Transforaminal epidural steroid injections deliver potent anti-inflammatory medication precisely to the S1 nerve root. Using fluoroscopic guidance, I advance a needle to the S1 neural foramen and inject corticosteroid combined with local anesthetic. This reduces inflammation around the compressed nerve, often providing significant pain relief that can last weeks to months.
Epidural injections are most effective when nerve root inflammation—rather than pure mechanical compression—is the primary pain driver. They can also serve a diagnostic role: if a selective S1 nerve root block temporarily abolishes symptoms, it confirms the S1 level as the pain generator.
The Discseel® Procedure
For patients with chronic S1 radiculopathy caused by L5-S1 disc pathology—specifically annular tears that allow inflammatory disc material to leak onto the nerve root—the Discseel® Procedure offers a regenerative approach.
As a Master Instructor trained directly by Dr. Kevin Pauza, the inventor of the Discseel® Procedure, I’ve performed this treatment for patients throughout Houston and Lawrenceville. The procedure involves injecting a biologic fibrin sealant into the damaged disc through a needle placed under fluoroscopic guidance. This sealant closes annular fissures, seals the disc’s outer layer, and promotes collagen regeneration within the annulus fibrosus.
By sealing the annular tear, the Discseel® Procedure addresses the underlying disc pathology causing S1 nerve irritation. Patients with confirmed annular tears on MRI and persistent S1 radiculopathy despite conservative care may be candidates for this minimally invasive, outpatient procedure. You can learn more about this treatment option through our Discseel® Video Resource Center.
Additional Interventional Options
Depending on the specific pathology, other interventional techniques may be appropriate:
- Selective nerve root blocks: Diagnostic and therapeutic injections targeting the S1 nerve root specifically.
- Spinal cord stimulation: For chronic, refractory S1 radicular pain, neuromodulation with spinal cord stimulators can provide significant relief by modulating pain signals before they reach the brain.
- Radiofrequency ablation: In select cases, thermal or pulsed radiofrequency applied to the dorsal root ganglion can reduce nerve-mediated pain.
Schedule Your Discseel® Consultation
Surgical Treatment
Surgery for S1 nerve compression is reserved for cases where:
- Progressive neurological deficits develop (worsening weakness or numbness)
- Cauda equina syndrome symptoms appear (bowel/bladder dysfunction—a surgical emergency)
- Conservative and interventional treatments fail to provide adequate relief after an appropriate trial
- Severe foraminal stenosis causes refractory symptoms
Surgical options include:
- Microdiscectomy: Removal of the herniated disc fragment compressing the S1 nerve root. This is a minimally invasive procedure with high success rates for relieving radicular leg pain.
- Laminotomy/foraminotomy: Enlarging the neural foramen by removing portions of bone or ligament to decompress the S1 nerve.
- Spinal fusion: In cases of instability or severe degenerative disease at L5-S1, fusion may be necessary to stabilize the segment and indirectly relieve nerve compression.
While surgery can be highly effective, it carries risks including infection, bleeding, nerve injury, and failed back surgery syndrome. I typically recommend exhausting conservative and interventional options before considering operative intervention.

Prevention and Long-Term Management of S1 Nerve Health
Preventing S1 nerve compression involves maintaining spinal health and addressing risk factors for disc degeneration. For patients who’ve recovered from an episode of S1 radiculopathy, long-term management focuses on preventing recurrence.
Core Strengthening and Lumbar Stabilization
A strong core musculature supports the lumbar spine and reduces stress on the L5-S1 disc. Physical therapy programs emphasizing core strengthening—targeting the transversus abdominis, multifidus, and paraspinal muscles—can improve spinal stability and reduce the risk of future disc herniation.
Exercises that promote neutral spine positioning during functional movements (lifting, bending, twisting) help protect the L5-S1 junction from excessive forces that can damage the disc and compress the S1 nerve root.
Posture and Ergonomics
Maintaining proper posture, particularly during prolonged sitting, reduces intradiscal pressure at L5-S1. Ergonomic adjustments—such as lumbar support in chairs, standing desk options, and frequent position changes—can minimize stress on the lumbosacral junction.
Avoiding prolonged forward-flexed postures (slouching, prolonged computer work without breaks) helps prevent disc degeneration and nerve compression.
Weight Management
Excess body weight increases mechanical load on the lumbar spine, particularly at the L5-S1 level. Weight reduction, when appropriate, can significantly decrease stress on discs and reduce the risk of nerve compression.
Activity Modification
For patients with a history of S1 radiculopathy, avoiding high-impact activities or heavy lifting that places excessive axial load on the spine is prudent. Low-impact aerobic exercise (swimming, cycling, walking) maintains cardiovascular fitness without overstressing the lumbar spine.
Conclusion: Understanding S1 Nerve Distribution for Better Outcomes
The S1 nerve plays a critical role in lower body motor function and sensation, controlling plantar flexion, providing feeling to the lateral foot and heel, and mediating the Achilles reflex. When compressed at the L5-S1 level—typically by disc herniation, foraminal stenosis, or degenerative changes—patients experience characteristic symptoms of S1 radiculopathy: radiating posterior leg pain, lateral foot numbness, weakness pushing off while walking, and reduced ankle reflexes.
Understanding S1 nerve distribution, pathway, and function helps patients recognize symptoms early and seek appropriate evaluation. While dermatomal maps provide a general guide, actual symptom patterns vary considerably among individuals, requiring careful clinical correlation with imaging findings.
Treatment begins with conservative management in most cases, progressing to interventional procedures when conservative care doesn’t provide adequate relief. For patients with chronic disc-related S1 radiculopathy, regenerative approaches like the Discseel® Procedure can address underlying annular pathology rather than just masking symptoms. Surgery remains an option for refractory cases or when progressive neurological deficits develop.
If you’re experiencing symptoms consistent with S1 nerve compression—radiating leg pain to the lateral foot, difficulty standing on tiptoes, numbness in the heel or outer foot—comprehensive evaluation can identify the source and guide appropriate treatment. At Performance Pain and Sports Medicine, we offer advanced diagnostic techniques and a full spectrum of treatment options, from conservative care through minimally invasive interventional procedures.
For patients in the Houston area, League City, Baytown, or Lawrenceville, New Jersey, you can schedule a consultation to discuss your symptoms and explore treatment options tailored to your specific condition.
This article is for educational purposes only and should not be used as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition or treatment options. Never disregard professional medical advice or delay in seeking it because of something you have read in this article.
Frequently Asked Questions
What is the S1 nerve distribution?
The S1 nerve distribution refers to the specific areas of your lower body that receive motor control and sensory innervation from the first sacral nerve root. This includes motor control of the calf muscles (gastrocnemius and soleus) for plantar flexion, as well as sensation to the lateral foot, fifth toe, heel, and sole. The S1 nerve also mediates the Achilles tendon reflex. When this nerve is compressed or damaged, symptoms appear in these specific distribution areas.
How do I know if my S1 nerve is compressed?
S1 nerve compression typically produces several characteristic symptoms: radiating pain from the lower back down the posterior thigh to the lateral foot and heel, numbness or tingling in the outer foot and fifth toe, weakness when standing on tiptoes or pushing off while walking, and a diminished or absent Achilles reflex. If you experience these symptoms, particularly if they worsen with sitting or bending forward, you should seek evaluation from a spine specialist who can perform a physical examination and order appropriate imaging to confirm S1 nerve compression.
Where does S1 nerve pain radiate?
S1 nerve pain typically radiates from the lower back or buttock region down the posterior (back) of the thigh, into the calf, and extends to the lateral (outer) aspect of the foot and heel. Some patients also feel pain or numbness in the sole of the foot and the fifth toe. The pain often follows the course of the sciatic nerve, which is why S1 radiculopathy is commonly associated with sciatica symptoms. However, pain distribution can vary between individuals and doesn’t always follow textbook dermatomal maps.
Can S1 nerve damage be reversed?
Whether S1 nerve damage can be reversed depends on the severity and duration of compression. Acute nerve compression from a disc herniation often improves with treatment—either conservative management or interventional procedures—as inflammation resolves and mechanical pressure is relieved. Many patients recover full function within weeks to months. However, prolonged or severe nerve compression can cause permanent damage (axonal degeneration) that may not fully reverse. Early intervention improves the chances of complete recovery. For chronic disc-related nerve irritation, procedures like the Discseel® Procedure can address underlying annular tears and potentially prevent ongoing nerve inflammation.
What is the difference between L5 and S1 nerve symptoms?
L5 and S1 nerve symptoms differ in their distribution patterns, motor findings, and reflex changes. L5 nerve compression affects the top of the foot and the big toe (dorsal foot), causes difficulty lifting the foot upward (foot drop), and typically doesn’t affect reflexes. In contrast, S1 nerve compression affects the lateral foot and fifth toe, causes weakness pushing the foot downward (difficulty with heel raises), and reduces or eliminates the Achilles reflex. Sensory symptoms also differ: L5 numbness occurs in the first web space between the big toe and second toe, while S1 numbness affects the lateral foot and heel.
What treatments are available for S1 nerve compression in Houston?
Houston patients with S1 nerve compression have access to comprehensive treatment options at Performance Pain and Sports Medicine. Conservative treatments include physical therapy, medications, and activity modification. When conservative care doesn’t provide adequate relief, interventional options include epidural steroid injections targeting the S1 nerve root and the Discseel® Procedure for patients with underlying disc pathology. As the first physician in Houston trained directly by the inventor of the Discseel® Procedure, Dr. Wiederholz offers this advanced regenerative treatment for appropriate candidates with chronic disc-related S1 radiculopathy. Visit our Houston location for specialized evaluation and treatment.















