By Dr. Matthias Wiederholz with Performance Pain and Sports Medicine
Quadruple Board-Certified in Physical Medicine & Rehabilitation, Sports Medicine, Pain Medicine, and Regenerative Medicine
Updated February 12, 2026
Medically reviewed and updated for accuracy
Quick Insights
A disc extrusion is a specific and more severe form of disc herniation in which the inner disc material (nucleus pulposus) breaks through the outer layer (annulus fibrosus) with a narrow base, extending into the spinal canal while remaining attached to the parent disc. Understanding the difference between a disc extrusion and other types of herniation, including protrusion and sequestration, helps guide accurate diagnosis and effective treatment planning.
Key Takeaways
- Disc herniation is an umbrella term that includes bulge, protrusion, extrusion, and sequestration, each with distinct structural features and clinical implications.
- In a disc extrusion, the displaced material extends beyond the annular defect with a base narrower than the dome of displaced tissue.
- Central disc extrusions may compress the thecal sac or cauda equina, while paracentral and foraminal extrusions tend to affect individual nerve roots.
- MRI is the gold standard for classifying herniation type, and accurate classification directly influences treatment decisions and prognosis.
- Disc extrusions may resorb naturally over time, but persistent symptoms or neurological changes warrant physician evaluation.
Why It Matters
Understanding the difference between disc extrusion and other herniation types empowers you to ask informed questions, interpret your MRI findings with confidence, and work with your physician to choose the most appropriate treatment. Misclassifying a disc extrusion as a simple bulge or protrusion can lead to delayed care, while overreacting to findings that may resolve on their own can lead to unnecessary procedures.
Introduction
As an interventional spine specialist with over two decades of experience treating disc conditions, I regularly help patients make sense of confusing MRI terminology. One of the most common questions I hear is: “What is a disc extrusion, and how is it different from a herniated disc?”
The short answer is that disc extrusion is a specific type of disc herniation. “Herniated disc” is a broad term that covers several categories of disc displacement, including protrusion, extrusion, and sequestration. A disc extrusion occurs when the soft inner core of a spinal disc pushes through a tear in the outer layer, with the displaced material forming a shape where the base is narrower than the dome. This distinction matters because different types of herniations carry different clinical implications, from symptom severity to treatment approach.
In this article, I break down the types of disc herniation, explain how extrusion differs from protrusion and sequestration, and outline the treatment options available for patients in Houston facing these conditions. If you are exploring advanced disc repair options, the Discseel® Video Resource Center provides an in-depth look at one of the minimally invasive approaches I offer for disc pathology.
What Is a Disc Extrusion?
A disc extrusion is a form of disc herniation in which the nucleus pulposus (the gel-like center of the disc) breaks through the annulus fibrosus (the tough outer ring) and extends into the spinal canal. According to a review in PMC on lumbar disc herniation morphology, the defining feature of an extrusion is that the height (or dome) of the displaced disc material exceeds the width of its base at the point of annular disruption.
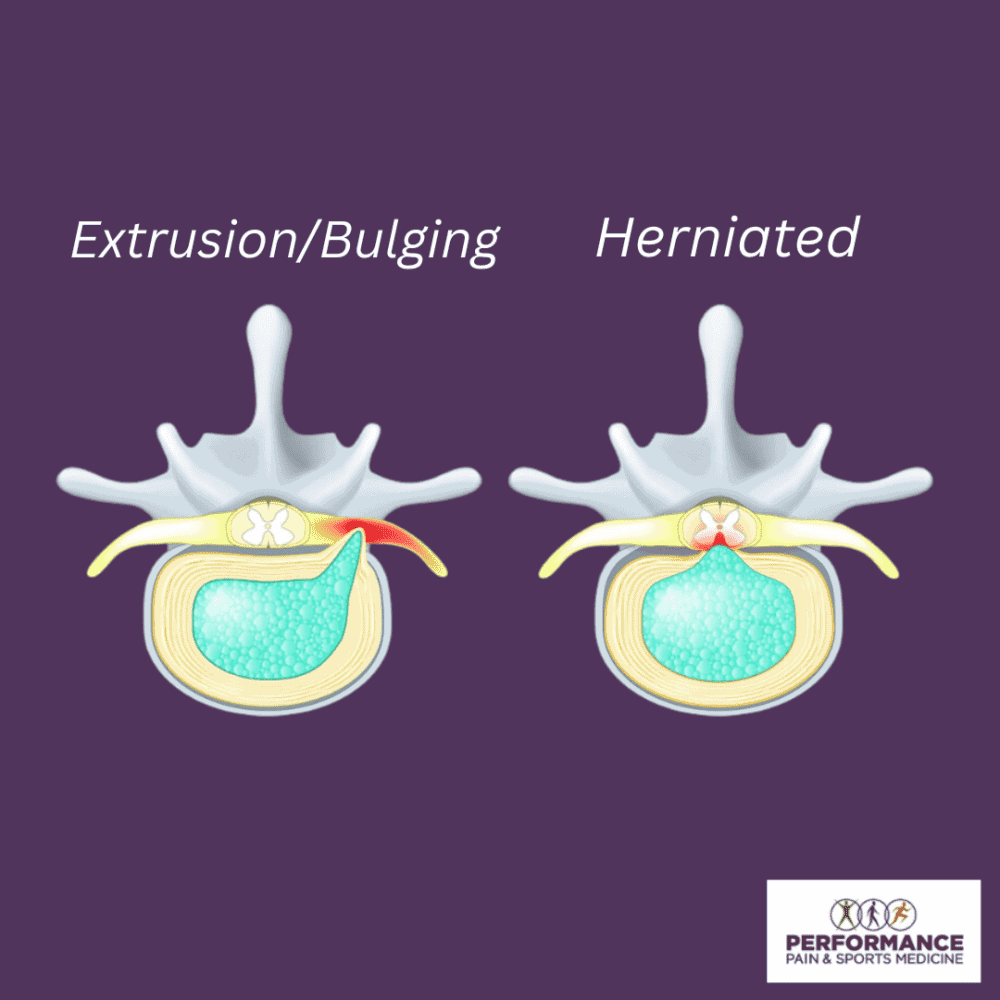
Think of it this way: if you squeeze a tube of toothpaste and the material comes out through a small opening and expands beyond that opening, the shape you see resembles an extrusion. The opening (the base) is narrow, while the material that has escaped (the dome) is wider. This is different from a protrusion, where the base remains broader than the displaced material.
Importantly, in a disc extrusion the escaped material remains connected to the parent disc. If that connection is lost and a fragment breaks free entirely, the condition is reclassified as a sequestration.
Types of Disc Herniation: Bulge, Protrusion, Extrusion, and Sequestration
Understanding the different types of disc herniation starts with recognizing that these terms describe a spectrum of disc displacement, each with increasing severity. The Spine Journal’s Lumbar Disc Nomenclature Version 2.0 established the consensus classification system used by spine specialists and radiologists worldwide.
A disc bulge is the mildest form. Here, the disc extends beyond the edges of the vertebral body in a generalized or circumferential pattern. The annulus fibrosus remains intact, and no focal displacement of disc material occurs. A bulge involves more than 25% of the disc circumference and is often considered a normal part of aging.
A disc protrusion represents a more localized displacement. In a protrusion, disc material pushes outward in a focal area, but the base of the displaced material (where it contacts the parent disc) is wider than the dome. The outer annular fibers may still be intact, or there may be a contained breach. Because the base is broad and the displacement is limited, protrusions are generally considered less severe than extrusions.
A disc extrusion involves a more significant disruption. The nucleus pulposus breaks through the annulus and extends into the spinal canal with a narrow base and a wider dome of displaced material. The material remains connected to the disc of origin. Extrusions carry a higher risk of nerve compression because the escaped material can press directly against spinal nerve roots or the thecal sac.
A disc sequestration is the most severe form. The extruded fragment loses all connection to the parent disc and becomes a free piece within the spinal canal. This “sequestered fragment” can migrate above or below the disc level, potentially compressing nerves at adjacent segments.
For a deeper look at how tears in the annulus fibrosus contribute to these conditions, our guide to spinal disc tears, causes, symptoms, and treatment options provides additional context.
Disc Extrusion vs Protrusion: How to Tell the Difference
The distinction between disc extrusion and disc protrusion comes down to shape and structural integrity. According to established spine nomenclature standards, the key differentiator is the relationship between the base and the dome of the displaced material.
In a protrusion, the base of the displaced disc material is wider than any other dimension of the displacement. The disc bulges outward but does not extend far beyond the annular defect. In many cases, the outer annular fibers may still partially contain the displaced material.
In an extrusion, the base is narrower than the dome. The disc material has pushed through the annulus more aggressively, creating a mushroom-like or teardrop-shaped displacement that extends into the spinal canal. This shape indicates a more complete breach of the annulus fibrosus.
| Feature | Protrusion | Extrusion |
|---|---|---|
| Base vs. Dome | Base wider than dome | Dome wider than base |
| Annulus Integrity | Partially intact or contained | Fully breached |
| Attachment to Disc | Connected | Connected (if sequestered, it is no longer an extrusion) |
| Severity | Mild to moderate | Moderate to severe |
| Nerve Compression Risk | Lower | Higher |
This distinction matters because extrusions are more likely to cause significant nerve compression, radiculopathy (radiating pain), and neurological symptoms like numbness or weakness. Protrusions, while they can certainly cause pain, tend to produce milder symptoms and often respond well to conservative treatment.
Central, Paracentral, and Foraminal Disc Extrusions
Beyond the type of herniation, the location of a disc extrusion within the spinal canal significantly affects which nerves are involved and what symptoms you experience. Research published in the Open Orthopaedics Journal describes how central disc extrusions produce different clinical presentations than lateral or foraminal extrusions.
A central disc extrusion occurs when the displaced material pushes directly backward into the center of the spinal canal. This type can compress the thecal sac (the membrane surrounding the spinal cord and cauda equina) and may affect multiple nerve roots simultaneously. In severe cases, a large central extrusion can cause cauda equina syndrome, a medical emergency characterized by loss of bladder or bowel control and saddle anesthesia (numbness in the groin and inner thighs).
A paracentral extrusion (also called posterolateral) is the most common pattern. The disc material displaces slightly to one side, compressing the traversing nerve root at that level. For example, a paracentral extrusion at L4-L5 typically affects the L5 nerve root, causing pain that radiates down the outer leg and into the top of the foot.
A foraminal extrusion pushes into the neural foramen, the bony opening through which nerve roots exit the spine. This type compresses the exiting nerve root rather than the traversing root. Foraminal extrusions can be particularly painful because the nerve is compressed within a confined space.
A far lateral (extraforaminal) extrusion extends beyond the foramen entirely, affecting nerve roots outside the spinal canal. These are less common but can be challenging to diagnose because they are easily missed on standard imaging views.
Disc Extrusion Symptoms and When to Seek Care
The symptoms of a disc extrusion depend on the location and size of the displaced material and which nerves are affected. Common symptoms include localized back or neck pain, radiating pain into the arms or legs (radiculopathy), numbness or tingling in the extremities, and muscle weakness in the areas supplied by the compressed nerve.
Patients with lumbar disc extrusions frequently describe sciatic-type pain that shoots from the lower back through the buttock and down one leg. Cervical extrusions can produce similar radiating symptoms into the shoulder, arm, and hand. The severity of symptoms often correlates with the degree of nerve compression, meaning extrusions tend to produce more intense symptoms than protrusions.
For a comprehensive overview of herniated disc presentations, our article on herniated disc symptoms, causes, and treatment covers additional details on recognizing these conditions.
When to Seek Emergency Care
Certain symptoms require immediate medical attention:
- Sudden loss of bladder or bowel control
- Progressive or severe weakness in both legs
- Numbness in the groin or inner thighs (saddle anesthesia)
These symptoms may indicate cauda equina syndrome or severe spinal cord compression, both of which require urgent evaluation.
How Disc Extrusions Are Diagnosed
Accurate diagnosis starts with a thorough clinical evaluation. During a neurological exam, I assess reflexes, muscle strength, sensation, and specific nerve tension signs (such as the straight leg raise test) to determine which nerve roots may be involved.
MRI is the gold standard imaging tool for distinguishing between types of disc herniation. An MRI shows the precise shape, size, and location of the displaced disc material, allowing the radiologist and treating physician to classify the herniation as a bulge, protrusion, extrusion, or sequestration. Research on MRI signal intensity correlates with herniation type has shown that imaging characteristics can even provide clues about how long the herniation has been present and whether it may be progressing or resolving.
In some cases, additional testing such as electromyography (EMG) and nerve conduction studies can help confirm which nerves are affected and assess the degree of nerve damage. Correct classification of the herniation type directly influences treatment recommendations, which is why seeking evaluation from a physician experienced in interpreting spine MRI is essential.
Treatment Options for Disc Extrusion
Disc extrusion treatment depends on the severity of symptoms, the degree of nerve compression, and how the condition responds to initial management. Most patients begin with conservative approaches and progress to more advanced interventions only when necessary.
Conservative care includes physical therapy, activity modification, and anti-inflammatory medications (NSAIDs). Many patients with disc extrusions experience meaningful improvement with structured physical therapy that focuses on core stabilization, nerve gliding exercises, and gradual return to activity. Short courses of oral steroids may help reduce acute inflammation around compressed nerve roots.
Epidural steroid injections can provide targeted relief when oral medications and therapy are insufficient. These injections deliver anti-inflammatory medication directly to the area surrounding the compressed nerve, reducing inflammation and pain. In my practice, I use fluoroscopic guidance to ensure precise placement.
Surgical options such as microdiscectomy or endoscopic discectomy may be recommended for patients with progressive neurological deficits, intractable pain, or symptoms that fail to improve with conservative treatment over 6 to 12 weeks. Surgery aims to remove the extruded disc material and decompress the affected nerve root.
Minimally invasive and regenerative options offer alternatives for patients who want to avoid traditional surgery. These include biologic disc repair procedures that target the underlying annular damage contributing to the extrusion.
The Discseel® Procedure: A Non-Surgical Option for Disc Extrusions in Houston
For patients with disc extrusions related to annular tears and chronic discogenic pain who want to avoid spinal fusion or discectomy, the Discseel® Procedure offers a non-surgical alternative. This outpatient procedure uses a biologic fibrin sealant to repair tears in the annulus fibrosus and promote natural collagen regeneration within the damaged disc.
I perform the Discseel® Procedure using fluoroscopic guidance. The process begins with a diagnostic annulogram to identify which discs have active tears and leakage. The fibrin sealant is then injected into the affected discs, where it seals the annular defects and creates an environment that supports tissue repair. Over time, the fibrin is absorbed and replaced with new collagen, restoring structural integrity to the disc.
Having been personally trained by Dr. Kevin Pauza, the inventor of the Discseel® Procedure, and as one of only a few certified master instructors worldwide, I have extensive experience with this technique. The Discseel® Procedure is designed for patients with documented annular tears who have not responded adequately to conservative care and want to preserve spinal mobility rather than undergo fusion. To learn more about the procedure and see patient outcomes, visit the Discseel® Video Resource Center.
If you are dealing with persistent disc pain from an extrusion or other disc pathology, see if you are a candidate for the Discseel® Procedure.
Prognosis and Natural Resorption of Disc Extrusions
One of the most encouraging findings in spine research is that disc extrusions have a higher rate of natural resorption than protrusions. The body’s immune system recognizes the extruded disc material as foreign tissue and gradually breaks it down through an inflammatory and enzymatic process. Over months, the displaced fragment can shrink or disappear entirely on follow-up MRI.
This does not mean that every extrusion will resolve on its own. Factors influencing resorption include the size of the extrusion, whether it has migrated away from the parent disc, and the patient’s overall inflammatory response. Larger extrusions and sequestered fragments tend to resorb more readily than smaller, contained protrusions, which may seem counterintuitive but is well documented in the literature.
For patients whose symptoms improve with conservative care, monitoring with repeat imaging can confirm whether resorption is occurring. For those whose symptoms persist despite conservative management, or who develop progressive neurological deficits, more active intervention is warranted. The key is working with a physician who can interpret your imaging findings in the context of your symptoms and guide treatment decisions accordingly.
Conclusion
The difference between disc extrusion and other forms of herniation comes down to the structural relationship between the displaced disc material and the annulus fibrosus. Understanding whether you have a bulge, protrusion, extrusion, or sequestration helps you and your physician determine the right treatment path. Disc extrusions carry a higher risk of nerve compression but also have favorable natural resorption potential in many cases.
Whether you need conservative management, targeted injections, or advanced options like the Discseel® Procedure, getting an accurate diagnosis is the essential first step. If you are experiencing persistent back or neck pain and want expert evaluation, see if you are a candidate for the Discseel® Procedure or contact our team to schedule a consultation.
Our Houston clinic provides comprehensive spine care, from initial evaluation and imaging interpretation through advanced interventional and regenerative treatments.
This article is for educational purposes only and should not be used as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition or treatment options. Never disregard professional medical advice or delay in seeking it because of something you have read in this article.
Frequently Asked Questions
Is a disc extrusion the same as a herniated disc?
A disc extrusion is one specific type of herniated disc. “Herniated disc” is a general term that includes protrusion, extrusion, and sequestration. An extrusion indicates that the inner disc material has broken through the outer layer with a narrow base and a wider dome of displaced tissue. It is considered more severe than a protrusion but less severe than a sequestration, where the fragment breaks free entirely.
What is the difference between disc extrusion and disc protrusion?
The primary difference is the shape of the displacement. In a protrusion, the base of the displaced material is wider than the dome, meaning the disc bulges outward but remains relatively contained. In an extrusion, the dome exceeds the base, indicating the material has pushed through the annulus more significantly. Extrusions typically carry a higher risk of nerve compression and more pronounced symptoms.
What is a central disc extrusion?
A central disc extrusion occurs when the displaced disc material pushes directly backward into the center of the spinal canal. This type can compress the thecal sac and potentially affect multiple nerve roots. Large central extrusions in the lumbar spine may lead to cauda equina syndrome, which requires urgent medical evaluation. Central extrusions differ from paracentral and foraminal extrusions, which affect nerve roots to one side or within the neural foramen.
Can a disc extrusion heal on its own?
Many disc extrusions do resorb naturally over time. The body’s immune response can gradually break down the extruded disc material, and follow-up MRI scans may show significant reduction or complete resolution. Larger extrusions and sequestered fragments tend to have higher resorption rates. However, not all extrusions resolve spontaneously, and persistent symptoms or progressive weakness should prompt evaluation by a spine specialist to determine whether intervention is needed.
How is a disc extrusion treated without surgery?
Non-surgical treatment for disc extrusion typically begins with physical therapy, anti-inflammatory medications, and activity modification. Epidural steroid injections can provide targeted relief for nerve-related pain. For patients with documented annular tears contributing to chronic disc pain, minimally invasive procedures like the Discseel® Procedure use biologic fibrin sealant to repair the damaged annulus and support natural disc healing without incisions or hardware.
When does a disc extrusion require surgery?
Surgery is typically considered when conservative treatment fails to provide adequate relief after 6 to 12 weeks, or when there are progressive neurological deficits such as worsening weakness, significant muscle atrophy, or signs of cauda equina syndrome. The specific surgical approach depends on the size, location, and characteristics of the extrusion, as well as the patient’s overall health and treatment goals. Many patients explore minimally invasive alternatives before committing to traditional surgery.















